Injectable Weight Loss Medications Before and After Bariatric Surgery
Wegovy® (semaglutide), Ozempic® (semaglutide) and Mounjaro® (tirzepatide)

How Effective are they ?
The graph below summarises typical average total body weight loss reported in major medication trials and commonly reported bariatric surgery outcomes. Medication and surgery data are not from head-to-head trials and should be interpreted as approximate comparisons only.
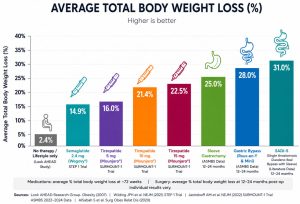
Figure 1. Average total body weight loss with no therapy / lifestyle only, semaglutide, tirzepatide and common bariatric procedures. Surgery outcomes vary by patient selection, operation type, follow-up duration and adherence to long-term care.
Use before bariatric surgery
In selected patients, injectable medications such as Wegovy® (semaglutide), Ozempic® (semaglutide) and Mounjaro® (tirzepatide) may be used before surgery to reduce operative risk and improve metabolic control.
- Shrink liver fat and liver size, improving surgical exposure during laparoscopic surgery
- Reduce intra-abdominal fat and technical difficulty
- Improve diabetes control, blood pressure and sleep apnoea
- Improve mobility and conditioning before surgery
- Potentially make surgery safer, easier and more likely to be successful
Use after bariatric surgery
Injectable medications such as Wegovy®, Ozempic® and Mounjaro® may also be highly effective after bariatric surgery. Many patients respond strongly after surgery because bariatric procedures already alter gut hormones, appetite signalling, insulin resistance and metabolic pathways. Combining surgery with GLP-1/GIP medications may therefore produce a synergistic effect.
- Weight regain after surgery
- Inadequate initial weight loss
- Recurrence of diabetes or metabolic risk factors
- Increased appetite, hunger or food cravings
- Long-term metabolic optimisation and weight maintenance
What happens when medication is stopped?
Obesity is usually a chronic relapsing disease. Published discontinuation studies show that stopping GLP-1/GIP medication therapy is commonly followed by clinically significant weight regain.
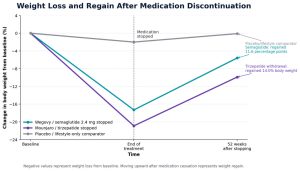
Figure 2. Weight loss and regain after discontinuation. The semaglutide line is based on STEP 1 extension data; the tirzepatide withdrawal line is based on SURMOUNT-4. The placebo/lifestyle comparator is shown for visual context and is not a direct head-to-head comparison.
Discontinuation data from the literature
| Medication stopped | Study | Key finding after withdrawal |
| Wegovy® / semaglutide 2.4 mg | STEP 1 extension | Average weight loss of 17.3% at treatment end; 11.6 percentage points regained over 52 weeks after stopping |
| Mounjaro® / tirzepatide | SURMOUNT-4 withdrawal trial | Average weight loss of 20.9% after 36 weeks; participants switched to placebo regained 14.0% body weight over the following 52 weeks; |
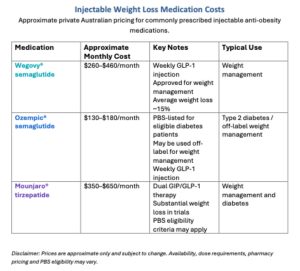
Cost considerations
These medicines can be expensive, and long-term therapy may be required. Costs vary by dose, pharmacy pricing, supply, PBS eligibility and private insurance arrangements.
For most patients, bariatric surgery provides a more durable and cost-effective long-term strategy, while medications may be used before surgery, after surgery or in combination with surgery as part of a personalised plan.
Risks and side effects
Common side effects include nausea, vomiting, reflux, constipation, diarrhoea, abdominal discomfort, fatigue and reduced appetite.
Less common but important risks include gallstone formation, dehydration, kidney injury, delayed gastric emptying, worsening reflux and pancreatitis.
Rare but increasingly reported complications include visual and eye-related problems.
International regulatory agencies have recently reviewed reports of:
Sudden irreversible visual changes due to rare irreversible optic nerve complications including non-arteritic anterior ischaemic optic neuropathy (NAION)
Any sudden visual change should be treated urgently.


Important considerations around surgery
Because these medicines slow gastric emptying, timing before anaesthesia must be discussed with George. Patients should also discuss diabetes medication adjustment, hydration, nutrition, pregnancy considerations and when to restart therapy after surgery.
Final message
Modern obesity care increasingly combines lifestyle therapy, nutrition support, behavioural care, injectable medications and bariatric surgery. For patients, combining bariatric surgery with injectable anti-obesity medications may provide powerful and durable improvements in weight, diabetes, cardiovascular risk, mobility, quality of life and long-term metabolic health. Treatment should always be individualised and supervised by an experienced multidisciplinary obesity and bariatric team that George leads at this Institute.